To detour around the block in this patient's C7 spinal cord injury and return hand function below the level of the injury, Mackinnon operated in the upper arms. There, the working nerves that connect above the injury and the non-working nerves that connect below the injury run parallel to each other, making it possible to tap into a functional nerve and direct those signals to a non-functional neighbor.
In this case, Mackinnon took a non-working nerve that controls the ability to pinch and plugged it into a working nerve that drives one of two muscles that flex the elbow. After the surgery, the bicep still flexes the elbow, but a second muscle, called the brachialis, that used to also provide elbow flexion, now bends the thumb and index finger.
"This is not a particularly expensive or overly complex surgery," Mackinnon says. "It's not a hand or a face transplant, for example. It's something we would like other surgeons around the country to do."

Surgeons at Washington University School of Medicine in St. Louis have restored some hand function in a quadriplegic patient with a spinal cord injury at the C7 vertebra, the lowest bone in the neck. Instead of operating on the spine itself, the surgeons rerouted working nerves in the upper arms.
(Photo Credit: Clark Bowen)
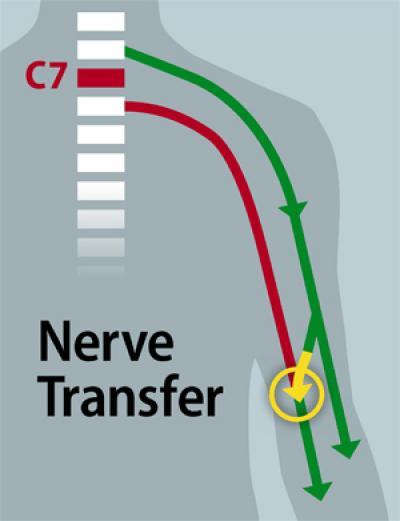
To detour around the block in this patient's C7 spinal cord injury and return hand function, Mackinnon operated in the upper arms. There, the working nerves that connect above the injury (green) and the non-working nerves that connect below the injury (red) run parallel to each other, making it possible to tap into a functional nerve and direct those signals to a non-functional neighbor (yellow arrow).
(Photo Credit: Eric Young)