Barcelona, Spain – Sunday 31 August 2014: Renal denervation reduces recurrent atrial fibrillation (AF) when performed with pulmonary vein isolation ablation in patients with AF and hypertension, according to research presented at ESC Congress today by Dr Alexander Romanov from the Russian Federation.
Dr Romanov said: "The prevalence of AF ranges from 1.5 to 2% in developed countries. This arrhythmia is associated with increased mortality, a five-fold risk of stroke and a 3-fold incidence of congestive heart failure. The vast majority of patients with AF also have arterial hypertension." (1)
He added: "Up to 10% of patients with arterial hypertension are resistant to modern drug treatment and have so-called resistant hypertension, which is associated with an increased risk of cardiovascular events." (2)
Renal sympathetic denervation (RD) is a new method that may be effective for controlling resistant hypertension by reducing the hyperactivity of the renal sympathetic nerve. In addition to its anti-hypertensive effects, RD may also exert antiarrhythmic effects, with reports suggesting a potential role for both AF and ventricular tachyarrhythmias. On the other hand, hypertension is an established risk factor for AF, and many cases of apparently "lone" AF (3) can be attributed to latent hypertension.
Pulmonary vein isolation (PVI) is a treatment for patients with AF. This catheter ablation technique uses radiofrequency energy to destroy tissue on the veins that is generating extra electrical signals and causing AF.
The aim of the present study was to assess the impact of adding RD as an adjunct to PVI in patients with AF and moderate or severe resistant hypertension (4) on AF recurrences and blood pressure changes.
The data for this analysis were obtained from two prospective randomised and double-blind studies. The analysis included 80 patients with a history of symptomatic drug refractory paroxysmal and persistent AF and moderate/severe resistant hypertension who underwent PVI and RD (figure 1) compared to PVI only.
The researchers found that RD reduced the likelihood of AF when performed with PVI in hypertensive patients. At 12 months follow up, 63% of the patients who had PVI and RD were AF-free compared to 41% of patients in the PVI only group.
The benefit was most dramatic in patients with severe drug resistant hypertension and those with persistent AF, although non-significant trends were also seen in patients with moderate hypertension and those with paroxysmal AF. Dr Romanov said: "We could speculate that the limited number of patients enrolled did not allow this trend to reach statistical significance. The use of RD in moderate hypertension as well as the effect on paroxysmal AF deserves further investigation."
RD delivered significant reductions in systolic and diastolic blood pressure. Dr Romanov said: "These results are compatible with those reported by previous trials in severe and moderate resistant hypertension. Moreover, in our study we used high frequency stimulation (5) for confirming the acute effect of RD. We believe this is a critical measure of success of this procedure."

This is the ESC Congress 2014 poster.
(Photo Credit: ESC)
He concluded: "We found that the addition of RD to PVI may be beneficial in patients with severe resistant hypertension and/or persistent AF. These results confirm our earlier findings but in a larger and more diverse cohort of patients. Additional and larger trials are needed to validate our results, and to assess the effects of combined treatment on maintenance of sinus rhythm and blood pressure control beyond one year.
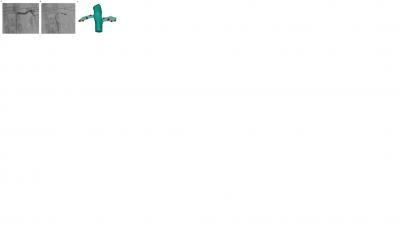
A. Angiography of the left renal artery; B. Renal ablation with the ablation catheter; C. Three-dimensional reconstructions with sites of radiofrequency ablation represented in red.
(Photo Credit: Dr. Alexander Romanov)
Source: European Society of Cardiology